Wait- masks that don't work on smoke-
magically work on Covid?

Is that possible? How?
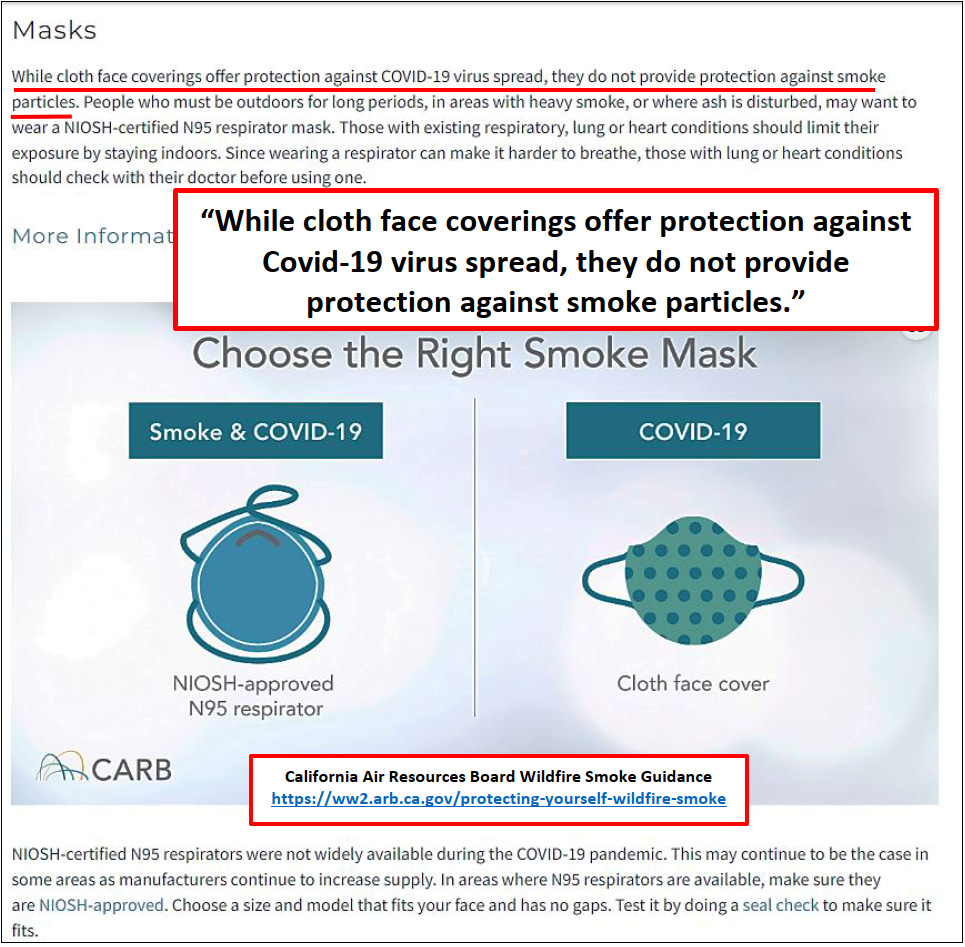
I wonder if the CARB page will be “updated” in the future. https://ww2.arb.ca.gov/protecting-yourself-wildfire-smoke
Imagine that you are a sincere CARB employee wanting to provide real, honest guidance about wildfire smoke to CA citizens, but also cannot contradict Covid 19 policy.
Strategic Communication, Masks, Public Health Noble Lies
One of the most effective persuasive communication techniques to an audience is when the countering party is inconsistent in their assertions or actions, as above.
I live in an area that is threatened by wildfire, at one point a couple years ago we were warned to be prepared to evacuate within 4 hours.
During that experience I ran across the Washington State Department of Health Wildfire Smoke guidance sheet, (below).
This guidance clearly states that nuisance dust masks and surgical masks, the same ones commonly seen for Covid policy compliance, are useless for wildfire smoke mitigation. N95 masks are described to be only potentially beneficial with multiple caveats regarding the difficulty of proper fit, use, and that many health conditions are a contraindication requiring consultation with a health care provider. With the admonition the N95 respirator should be used the minimum amount of time necessary.
There is certainly no claim that an N95 can be worn for a complete workday or school day, much less for weeks, months, and years. Most importantly, it clearly discloses that “Masks are not approved for children.” This guidance was dated July 2019, one year prior to the required masking of everyone, with the Covid order not even calling for masks but for “face coverings”.
Face coverings with no criteria whatsoever.
During the “Shelter in Place”, “Stay Safe at Home”, “2 Weeks to Flatten the Spread” disaster I dove into the WA state emergency planning, (This will be in future posts).
I reviewed the WA DOH Non-Pharmaceutical Implementation, NPI, Guidance manual produced on 2.29.2020. There are 13 possible NPI’s, ranging from “increase handwashing and use of alcohol-based sanitizer” to “establishing a cordon sanitaire”, and masking is not included or even mentioned as a potential intervention.
To try to understand where masking originated, I dug further into the source documents in the Washington Comprehensive Emergency Plan.
https://mil.wa.gov/asset/610b03295e5b4
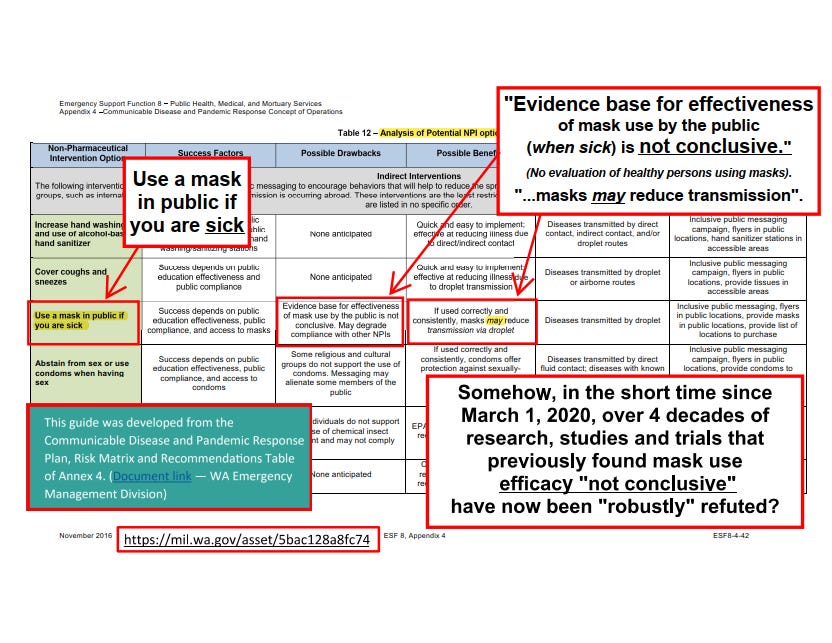
I located a table evaluating masks as an intervention and why it was not included.
“Possible Intervention”: “Use a mask in public if you are sick.”
“Possible Drawback”: “Evidence base for effectiveness of mask use by the public is not conclusive. May degrade compliance with other NPIs."
"Possible Benefits”: “if used correctly and consistently, masks may reduce transmission via droplet.”
So how did the Washington State Department of Health make an about face from “Masks are not approved for children”, and reviewing and rejecting masking as a possible intervention due to ineffectiveness for an aerosolized virus, to requiring children to wear unapproved masks all day every day in schools? And for the public in all other places? https://doh.wa.gov/sites/default/files/legacy/Documents/Pubs//334-353.pdf
And now, how does a Public Health agency go forward after giving inaccurate information? If a Paw Patrol cloth mask purchased from Etsy can prevent the inhalation of an aerosolized virus it should be effective on wildfire smoke, shouldn’t it?
Look at that gem from the California Air Resources Board website guidance on wildfire smoke. “Masks: While cloth face coverings offer protection against COVID-19 virus spread, they do not provide protection against smoke particles.” Excuse me?
Enter the “Noble Lie”. I will upload a slightly extended version of a piece I composed for The Flame USA newspaper exploring that subject in a future post. https://theflameusa.com/
“But masks must help a little?”
Population based masking is premised on several fallacies- one is that “face coverings” can act as source control- keeping virus “in”, or protective- keeping virus “out”. With the face coverings that most people use, and the manner in which they are used, they are virtually ineffective at either task. A properly fitted N95 mask used by a trained health care provider in a clinical setting, applied in a sanitary fashion, during exposure time in a treatment room with an ill patient, then properly removed in a sanitary fashion and disposed of or sterilized after use, potentially does have some efficacy. Contrast that to observed population-based masking practices.
But the other largely false premise is that there is widespread asymptomatic transmission. If there was widespread asymptomatic spread, then a) you would be masking yourself for the purpose of source control because you don’t know you are actively contagiously sick and don’t want to unintentionally expose others, and b) because other people you interact with don’t know that they are actively contagiously sick, and your mask is to prevent them from unintentionally exposing you.
But if there is little or no asymptomatic spread then masks can’t work, even if they did work, because if there is no unknown infection to source control or prevent, there is therefore no source control or prevention to be achieved.
It almost feels like a Zen koan:
“Even if masks worked, if there is no asymptomatic spread, they can’t work, because there is nothing for the mask to work on”.
In a conversation with a well-intentioned, but rabid masker they asked, “Surely if it captures a droplet, that will interrupt transmission, won’t it?” That is a legitimate question from a person seeking to understand and explain why trusted health authorities would require an “inconclusively effective” intervention.
My reply in a personal communication:
“I understand that it seems intuitive that masks should provide some value, I believed there was more efficacy prior to my research. But masks really can’t help because of the near molecular behavior of the radical small, aerosolized virus particulates. Tiny particles are more dangerous than drops, and the particles can stay aloft for hours. When inhaled they travel in the center of the air column and can penetrate deeper into the lungs. Droplets are subject to gravity, will descend to the floor, and are more easily countered by the nasopharyngeal system if ingested.
In the instances when a larger drop is caught in mask, if a person removed that mask and replaced it in a sanitary fashion, like a tissue, there could be some value for having contained a droplet. But, if the mask is retained, then breathing through the drop has the potential to evaporate or nebulize the more controllable larger droplet into smaller, more active particles that can penetrate the mask material and suspend in the air near indefinitely. Nebulizing viruses is a normal laboratory practice in animal viral testing, to facilitate the virus reaching the lower alveoli and increase infectivity. The nebulizing process is achieved largely by suspending an infective droplet in a membrane in front of a pneumatic source. https://www.niaid.nih.gov/research/aerobiology-integrated-research-facility https://www.biorxiv.org/content/10.1101/594358v1.full.pdf ”
Below is a tweet I prepared to hopefully help educate a blue check who was surprised at the controversy over the effectiveness and appropriateness of masking children in schools.







https://doh.wa.gov/sites/default/files/legacy/Documents/Pubs//334-353.pdf



https://mil.wa.gov/asset/610b03295e5b4