

Texas Measles Hospital CEO:
“But it’s not a terribly lethal disease.”

There is a fascinating interview with Albert Pilkington, CEO of the Seminole Hospital District in the heart of Gaines County, the epicenter of the Texas measles outbreak.
Audio available at this link:

Mr. Pilkington is not buying into the fear-porn of measles being an existential threat to Texas and the US.
“But it’s not a terribly lethal disease. I mean, there are cases, but, you know, relative to the amount of people that used to get measles, how many would pass away? You know, it’s not like a swine flu or anything like that. So, I mean, we respect everyone’s right to vaccinate or not get vaccinated. I mean, I think that’s just that’s what it means to be an American, right?”
“And so, you know, what we stand ready to do is do everything we can to help them get through the process, just like we help(ed?) people get through the process before we had a vaccine.”
___________________________________________________________________________
Interview transcript copied below:
“At the epicenter of the West Texas measles outbreak, one hospital in Gaines County works towards containment.”
“Seminole’s Mennonite community generally take religious exemptions from vaccinations. This has left them, and especially the children, vulnerable to the disease.”
Texas Standard: How does a rural hospital like yours prepare for such a rapidly growing outbreak?
Albert Pilkington: Well, you know, we got a little practice with COVID.
You know, it’s not as big of a deal as what somebody from the outside of health care might think. I mean, we’ve been doing disaster preparedness and dealing with all kinds of chaotic events since the beginning of, I guess, organized health care.
And so, it’s not as tough for us, really. We instituted our protection protocols for our employees and to cut down the cross examination (contamination?) probably within about 12 hours when we realized we’re starting to have a trend of cases.
Well, let’s talk about the patients. How are these cases being treated? I mean, this is very contagious.
Very contagious. I think that it’s the one of the most contagious diseases that’s out there. Fortunately, it has fairly low lethal component to it. But it’s quite contagious.
And so, you really have to follow the same protection protocols as you would with COVID – you know, contact precautions, masks. And so that’s kind of the big issue for it.
It’s very contagious, and you got a population that lives fairly close to us, a religious community of Mennonites, that, you know, they don’t believe in putting anything foreign into their body. And so that falls within the avenue of vaccines. And so, you know, once the disease process starts with one person, then let’s say it’s like a fire on a bunch of dry hay, it kind of burns through pretty quick.
So, tell me about what you’ve seen at your hospital.
Youth. I mean, primarily youth. We’ve shipped, I think, about 3 or 4 patients out that were really young – spiking a high temperature. So, we went ahead to be cautious and sent them up to the children’s hospital in Lubbock.
And then we’ve had about 13 hospitalizations ourselves. And basically, you’re trying to keep them hydrated, keep their fevers down and stuff like that. You know, that’s really what I’ve kind of done.
But it’s not a terribly lethal disease. I mean, there are cases, but, you know, relative to the amount of people that used to get measles, how many would pass away? You know, it’s not like a swine flu or anything like that. So, I mean, we respect everyone’s right to vaccinate or not get vaccinated. I mean, I think that’s just that’s what it means to be an American, right?
And so, you know, what we stand ready to do is do everything we can to help them get through the process, just like we help people get through the process before we had a vaccine.
So, clearly, you want people to be cautious. It can be serious for some people.
It can be. Especially youth, especially children. Yes.
Well, let’s talk about the Mennonite population. This outbreak is particularly hitting this population hard. What kind of outreach or resources are there in these communities?
Well, you know, of course we’re here. And so, we’re always available. I think we’re the spear point of this whole process. I think we’ve had 42 cases and the entire region’s had like 48 cases. And so, we’ve reached out to them quite a bit.
You know, what we have done is offered – with support of UMC, which is the University Medical Center up in Lubbock – they have a, for lack of a better term, a clinic bus. It’s a large Greyhound that has a mobile clinic activities, and they brought it down and put it in our parking lot to help us with doing titers and stuff to finding out who has immunities and who doesn’t. So, we’ve made that publicly available to everybody. That way you at least know are you at risk or are you not at risk?
And we offer vaccines. But, you know, I don’t believe their standards would allow them to be able to do the vaccines. But we have tried to provide them with as much as we could to insulate them from cross-contamination.
So, what can be done to help stop the spread of the disease in the area? You mentioned vaccines. Of course, high number of people unvaccinated – Mennonites, but others. So, what can you do?
Well, short of isolation, there’s not much you can do. I mean, as we mentioned earlier, it’s an extremely contagious disease. I mean, it’s probably a top five. It’s not a top three. Very contagious.
And so, I mean, if you roll back a couple of hundred years or so, I mean, it’s some of the things that wiped out some of the initial Native American populations in America. Because what comes along with it is a real high fever and everything. And, you know, you don’t have a way to treat the fever, it’s kind of a risk.
And so if you’re not going to do the vaccines and stuff, your choices are essentially isolation until basically you come across someone in your life that does have it and you’ll get infected. The other thing is you’ve got to keep the fevers down. If you have a particularly young child and the fever is very high for a long period of time, then you can begin to have neurological damage, ranging from hearing loss side to other associated neurological problems.
And I think that’s if you’re not going to do the vaccine, you definitely have to do everything you can. If you get infected, keep the fever down.”
_______________________________________________________________________
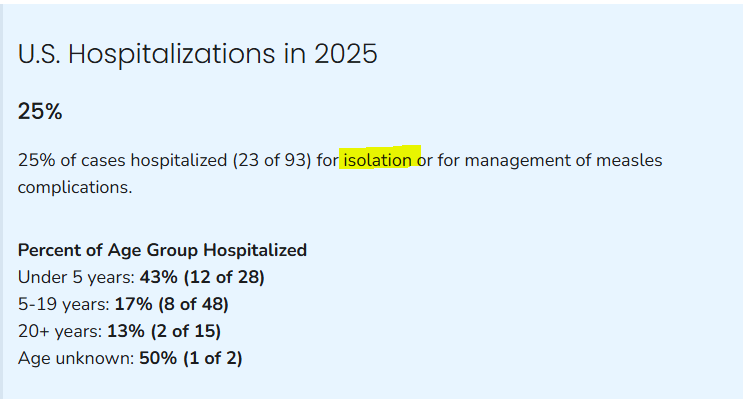
What about the hospitalization rate?
Per the CDC, patients with mild cases are being hospitalized for isolation purposes.
This is not SOC- “Standard of Care”.
Me and my siblings and mother all got the measles in the early 1960s. This wasn't a big deal. I got mumps a few years later; aside from missing the class outing to a local zoo, it was just a few days of discomfort accompanied by ice cream.
I don't know why they never mention the switch to a LIVE virus in 1968 - the live attenuated MMR vaccine, measles, mumps, and rubella viruses or the MMRV which adds live varicella virus. These live virus vaccines almost always lead to at least a measles outbreak, because not every body can handle even the weakened live virus. Anyone immuno compromised, or their household members, or with severe allergies, or who is around pregnant ladies - none of these kids should get a live virus vaccine. And how many kids are given a shot who don't KNOW they have compromised immune systems? In 1978 I was required to get the MMR at age 13 to attend school. Within 10 days I had a huge case of the big red measles. Who all did I expose in those 10 days before being diagnosed? We were told we were lucky it wasn't the German measles.
Many years later, after some horrible health issues, at 41 we learn I have Rheumatoid Arthritis; if we had known to check when I was 13, we would have known to not get any live vaccines, but I had no symptoms at 13, nor were my parents or I questioned about family members with issues (my Dad) or even if I was around any pregnant women (I was). How many other kids have compromised immune systems or allergies and are being required to get these live vaccines? And unknowingly spreading/causing outbreaks? The public health departments know this, but you don't ever hear about it. Why?
You look at any measles outbreak in the US since 1968, I guarantee there was a vaccination with live attenuated MMR before it started. Including the recent one in TX.